Ebola Outbreak in the DRC: A Complex Public Health Challenge

Residents gather to inspect the remains of a burnt medical tent at the General Referral Hospital of Mongbwalu in Mongbwalu, on May 23. The international response in eastern DRC will succeed or fail on its ability to implement emergency public health measures within the region’s long-standing social, political, and security quagmire, says the writer.
Image: AFP
Dirk Druet
On May 15, 2026, the Democratic Republic of the Congo (DRC) confirmed its 17th recorded outbreak of Ebola in Ituri province.
Since then, the number of cases has risen to over 900, and the virus has crossed into Uganda and reached the provinces of North and South Kivu, now controlled by the Rwanda-backed M23. Initial reports suggested that the outbreak may have been circulating for weeks, and local health authorities were underprepared to swiftly mount a containment strategy.
As international concern grows that the deadly virus might be out of control, the mounting public health response is facing an even more challenging environment than during the last major outbreak in 2018.
No vaccine exists for this strain of the virus, and Goma, the logistical hub of eastern DRC, is occupied by an armed group. The UN peacekeeping operation in the DRC (MONUSCO) has been drawing down its operations and is now confined to Ituri and North Kivu.
On top of this, the global health architecture is under strain following the US withdrawal from the World Health Organisation (WHO) earlier this year and a growing deficit in funding to address health emergencies. In this challenging and high-risk context, the lessons of the last outbreak must inform the management of this one.
The temptation in a fast-moving outbreak is to treat the response as an urgent technical problem requiring an urgent technical solution: identify cases, trace contacts, isolate the infected, vaccinate where possible, and bury the deceased safely.
But as many learned during the COVID-19 pandemic, emergency health responses in complex political situations are not neutral interventions in passive contexts; they are political acts. This is particularly true in conflict environments, where large-scale public health responses distribute resources at scale, legitimise or delegitimise particular actors, reshape local security arrangements, and engage with populations that read them through the lens of the conflict.
When the Health Response Became Part of the Conflict in the DRC
In eastern DRC, the 2018–2020 Ebola outbreak was described by WHO as a “perfect storm” in which a highly infectious disease was spreading in an area of active conflict.
The Congolese public, particularly in the country’s east, widely viewed their government as predatory, and much of the affected population resided in crowded conditions with poor health infrastructure and was located near porous international borders.
Given the seriousness of the risks to local and international public health, WHO and partners in the international community launched a massive health and humanitarian response. This operation was grounded in the principle of “no regrets,” which holds that it is better to overreact to a public health emergency and adjust later rather than act too late.
This approach was broadly seen as empowering the WHO to take direct action in the affected area with only limited consultation with other parts of the UN system.
Many of the decisions made during this period had devastating side effects: they empowered officials and security forces notorious for reprisals against local communities and produced what became known as the “Ebola Business”—a war economy with actors invested in prolonging the crisis.
This conflation of the Ebola response with the conflict led to community resistance and violence against health workers that inhibited containment and accelerated transmission. By the time the outbreak was declared over in 2020, more than 3,400 people had been infected, of whom some 2,200 had died.
Moreover, the conflict in eastern DRC had become even more entrenched, with the ADF armed group carrying out sustained atrocities in Beni territory in North Kivu. MONUSCO’s authority was openly contested by host populations, culminating in the torching of its office in Boikene, near the town of Beni, in 2019.
The risks to Congolese lives and international public health posed by the latest outbreak merit a large, swift health and humanitarian response. Such a response is all the more urgent following recent cuts to international support to the Congolese national health system, particularly as a result of the dismantling of USAID, which has reduced the country’s epidemic preparedness and likely undermined its capacity for early detection.
However, a response that is not grounded in an understanding of conflict dynamics is likely to hamper efforts to stem transmission. In a 2022 study for the American Academy of Arts and Sciences, I analysed the national and international response to the 2018–2020 outbreak and proposed a variety of ways international responders could have done things differently.
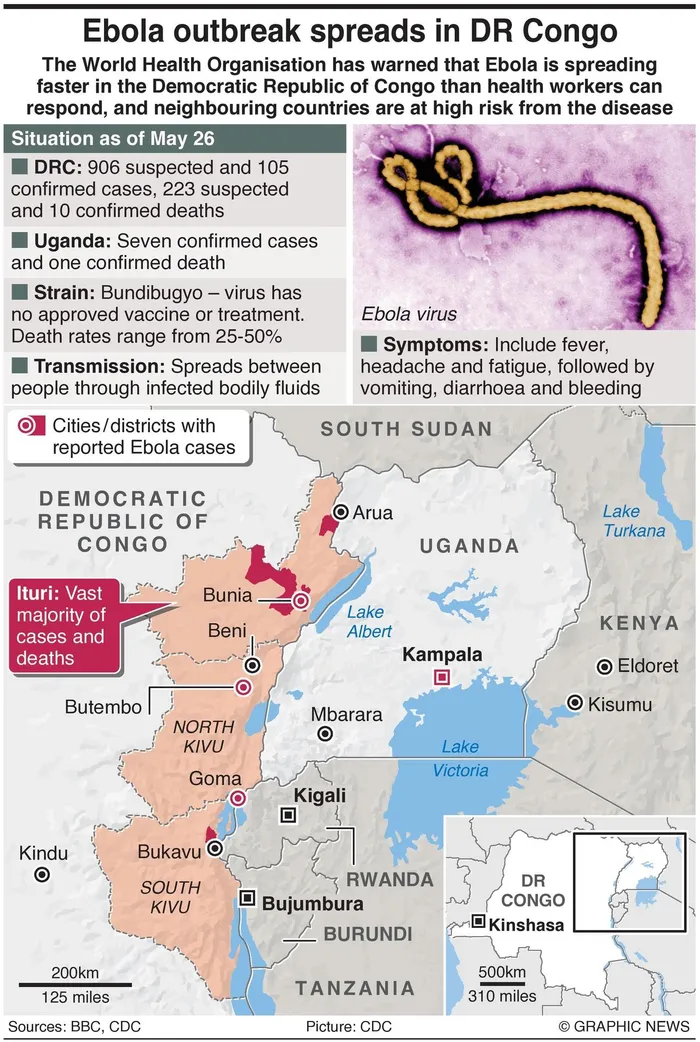
The spread of the latest outbreak of Ebola in the DRC and neighbouring countries.
Image: Graphic News
Three recommendations from that study remain relevant for the current outbreak:
- Treat conflict and political economy analysis as central to the design of the health response: In 2018, WHO did not request MONUSCO’s analysis of the security and political landscape into which it was deploying, and MONUSCO was not informed in advance of several key WHO decisions. That arrangement, documented by the Congo Research Group, created perverse incentives, securitised the response, and lowered public trust in the health response.
- Position peace and security actors at arm’s length from health activities: There is a critical distinction between using security actors to provide a generally permissive security environment for a health response and using them to provide direct, proximate security. Using uniformed personnel to escort vehicles, guard clinic perimeters, or cordon off health facilities changes the character of the intervention in the eyes of affected communities. While MONUSCO and national security services may have a role in promoting security during the health response, they should clearly distinguish themselves from humanitarian and health operations.
- Balance the urgency of epidemic response with community engagement and operational flexibility: The “no regrets” posture that prevailed in 2018 produced the conditions that ultimately undermined its effectiveness. Public health measures only function if affected populations trust them enough to participate; securitised responses that treat communities as obstacles rather than partners are counterproductive.
WHO’s Global Health and Peace Initiative, and Its Limits
To its credit, WHO has not ignored the 2018–2020 experience. In the years following the outbreak, the organization developed the Global Health and Peace Initiative (GHPI), built around two pillars: (1) making health programming “conflict-sensitive” by extending the “do no harm” principle into operational practice and
(2) where conditions allow, making it “peace-responsive” by designing health interventions to actively contribute to peace outcomes such as social cohesion, dialogue, and community resilience. The initiative is likely to influence WHO’s thinking as it rapidly designs and rolls out its response to the current crisis.
Two in particular could present challenges for the response in eastern DRC.
First, it is unclear how WHO and its partners in the field, including organisations such as Médecins Sans Frontières, will reconcile the principles of conflict sensitivity and humanitarian impartiality when the two pull in opposing directions. The GHPI offers no framework for managing that tradeoff.
Second, the initiative holds that programming “must be led at the national level—from national authorities down to the community level.” This instinct to promote national ownership was borne of the lessons of the 2014-2016 Ebola crisis in West Africa, where the UN was criticised for bypassing national institutions.
However, this principle becomes highly problematic when the state is itself a party to the conflict. The outbreak in the DRC demands a more localised, nuanced process for deciding on the role of national actors, grounded in thorough conflict analysis.
The Way Forward
The international response in eastern DRC will succeed or fail—and it must succeed—on its ability to implement emergency public health measures within the region’s long-standing social, political, and security quagmire.
This will require three deliberate moves from the outset:
(1) joint conflict and political-economy analysis to shape deployment decisions rather than follow them;
(2) a security posture of less proximate protection combined with negotiated community-level access; and
(3) a response built on localised approaches to engaging existing community structures and calibrating the role of national actors.
The decisions international responders make in the next weeks could have profound implications for regional and international public health.
* Dirk Druet is a Non-resident Senior Adviser at IPI. He is an Adjunct Professor McGill University’s Max Bell School of Public Policy and has served in several headquarters and field positions in the UN. This is a lightly edited version of the article published at https://theglobalobservatory.org/
** The views expressed do not necessarily reflect the views of IOL or Independent Media.